
A Look at Why Things Changed
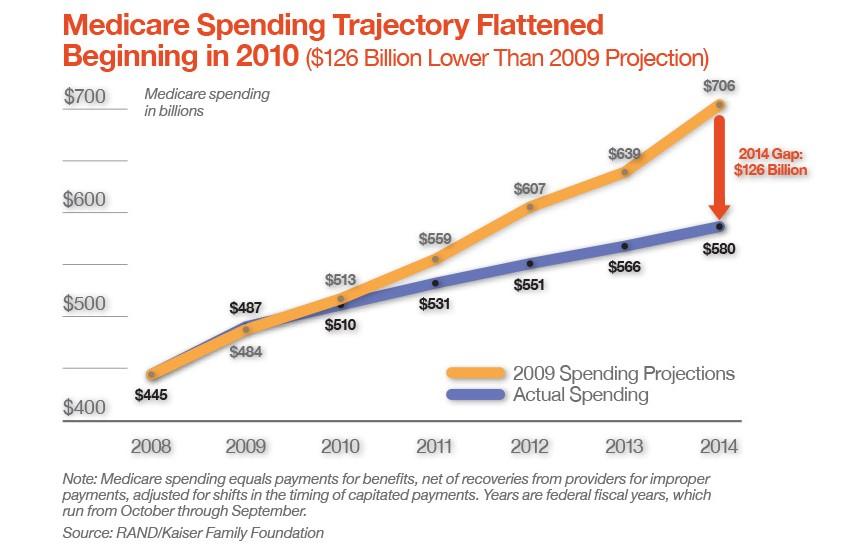
Editor's Note: A stable and progressively designed Medicare program is clearly one key to supporting the long-term health and lifestyle needs of Coloradans. More than 775,000 people in Colorado - mostly seniors, but some younger people with qualifying conditions - get their health coverage and care through the federal Medicare program. For years, analysts sounded deafening alarms about the retirement of baby boomers pushing Medicare into insolvency and destroying the federal budget. In 2014 and 2015, updates from actuaries showed a stunning turnaround: Medicare was getting healthier. Per capita Medicare spending not only flattened out in 2009, it actually dropped slightly after 2011 - an unprecedented development in a program accustomed to the buffeting of high medical inflation. In real dollars, the savings are in the hundreds of billions: Actual Medicare spending in 2014 was $580 billion, while as recently as 2009 the projection for that year foresaw $706 billion in spending. We asked Kaiser Family Foundation health care analyst Juliette Cubanski to walk us through how and why Medicare’s outlook has changed. Cubanski, of Menlo Park, Calif., is associate director of the Program on Medicare Policy at KFF.
Before the recent, more optimistic analyses of the Medicare spending slowdown, what had been the worries and the predictions about the program and its supposedly untenable costs?
It boils down to a simple fact of demographics of the population aging: the sheer number of people coming onto the program, aging onto Medicare eligibility when they turn 65. The growth in that population has been a cause for great concern; holding everything else constant, if there were more people coming onto the program and the per capita costs were growing at the rates they had historically, there were real concerns about Medicare having a shortfall in financing. The problem is that the rate of population aging is outpacing the rate at which we are growing the worker base. So there have been some pretty serious and dire projections of Medicare not having enough money to pay for all the hospital benefits that would come due in a relatively short period of time.
In 2009, just six years ago, the Medicare trustees were projecting that the Medicare hospital insurance trust fund, where all these payroll benefits go, was going to basically run out of money and not have enough money to pay current hospital bills as soon as 2017. That was really just right around the corner then. That was the big picture.
We keep hearing the statistic that boomers are turning 65 at the rate of 10,000 to 11,000 a day. Shouldn't that alone threaten the system?
That started in 2011, when the baby boom generation started turning 65. Prior to then, the population growth had been a coming concern, but it hadn’t come yet. After 2011 is when that number you tossed out became a reality. This baby boom population that is going to last for 20 years is really just now coming into Medicare eligibility.
And so financially for the Medicare system, what has happened instead of those more dire projections?
One point of comparison: I mentioned in 2009 the trustees were projecting the date of insolvency would be 2017; now in their most recent report for 2015, they are projecting the insolvency date is pushed out to 2030. That’s one clear indicator of Medicare's improved financial health.
So instead of eight years of solvency, we have at least 15 years of solvency?
That's right. So there we have a clear indicator that Medicare spending projections are not completely under control, but certainly more under control than they were five or six years ago.
So what have you and other analysts found as you've dug into the numbers? Why are costs not rising as fast as predicted?
In our 2014 paper, we tried to look at what happened that year. There are some obvious explanatory factors, some not so obvious and some residual results which we cannot explain. The obvious reason is that the (Affordable Care Act) passed, and that included many provisions affecting the Medicare program and Medicare spending. They were implemented as early as 2011; others rolled out over time. There were basically provider payment cuts and the rate at which those payments were allowed to grow over time. That was one obvious and immediate way to bring Medicare spending under more control – by cutting them now and building into legislation future constraints on the rate of growth going forward.
The hope among supporters of the reforms is that these efforts will take hold and more people will get behind them ... and that the system will change in such a way that we don't need a full-scale restructuring of the Medicare program.
Another big factor is the reduction in payments to Medicare Advantage programs, the managed care counterpart to traditional Medicare. Historically they have been paid more to provide the same benefits; that plan got paid more than if the person had stayed in traditional Medicare. Some legislators had been bothered by this for years, and they were finally able to restructure and level the playing field. It's phasing in over time.
Can any of the flattening of growth be attributed to various spending and care experiments going on around the nation in Medicare?
There are some other provisions in the ACA that might be contributing factors, but we can’t assign dollar savings to them because it’s too early to tell what role, if any, they are playing. Things like (accountable care organizations), Medicare Shared Savings, bundled payments, independence at home programs – a lot of these initiatives and demos and pilots are being rolled out in various places. It’s really hard at this relatively early stage of the game to evaluate how successful these are. I would say some have showed modest signs of promise, but it’s tens or hundreds of millions in savings versus an overall program that spends hundreds of billions. They would have to be rolled out on a much larger scale in many more parts of the country.
The chart on the first page of your 2014 report shows the flattening of per capita patient spending in recent years. Is that significant?
It's definitely a big deal. Historically, per capita spending has just gone up, and I think people expected that as a fact and not something you could really do much to change. So the fact that spending trend has been relatively flat is really unprecedented in Medicare. There are some other changes, besides the experimentation I mentioned, that could be significant. For example, growth in prescription drug spending has been much lower per person than it had historically. While prescription drugs are only about 10 percent of Medicare spending, that trend line does have an effect on the overall Medicare trend line. More people were shifting to generic drugs; fewer blockbuster brand name drugs (were) being introduced. And a lot of the more popular brand name drugs lost patent protection and had generics become available.
There are some other things possibly related to delivery system reform. There have been large relative reductions in the hospital readmission rate. Hospital spending is roughly about one-quarter of annual Medicare spending, so there's a lot of money involved, and clearly Medicare would be happy to see a successful effort in this area.
What is commonly referred to as waste, fraud and abuse - (Medicare has) tried a lot of things in recent years. One area is home health spending, some pretty egregious examples of fraudulent providers; (Medicare's) efforts have been pretty successful, according to the Office of Inspector General and others.
I'm sure lawmakers want to know if all of this tightening of the screws has changed consumer satisfaction or quality ratings for the worse.
We don't focus on that so much at Kaiser, but I'd say the quality measures that have been around for a while, I haven't seen any indication that quality of care has suffered as a result of these initiatives. If anything, Medicare may be sorting out the good from the bad in these integrity efforts. It's very difficult to find evidence that access to care has been affected negatively by any of these efforts. Most people say they are very satisfied with Medicare and that really hasn't changed much at all over the history of Medicare or the history of us asking that question.
Has the flattening of costs changed the tenor of the long-term debate about Medicare?
Yes and no. I think it depends on who you are listening to. There are some policymakers who are paying more attention to recent news about what’s happening with Medicare spending and see this as evidence of the effectiveness of the ACA and payment reform, and many people want to double down on those reforms and go bigger and go bolder with those initiatives. But other policymakers seem to not be paying much attention to Medicare's recent history and are talking about raising Medicare's eligibility age and benefit design and shifting to the premium support model. Those ideas are designed to address what might be seen as Medicare's long-run problem: The aging of the population is happening. No matter what you do to Medicare now, the fact is we are going to have upwards of 80 to 90 million people on Medicare in a few decades. And that is the reality that I think many people feel has still not been addressed.
The hope among supporters of the reforms is that these efforts will take hold and more people will get behind them, and as providers get more used to living with bundled payments and the experiments take hold, that the system will change in such a way that we don't need a full-scale restructuring of the Medicare program. There are still some people who are very philosophically opposed to Medicare as it exists today and want it to be a different program in the future.
There are kind of two realities going on for policymakers, depending on which side of the aisle you're on: the vision you have for the health care system overall and where you see Medicare fitting in.
This article was originally published in the Fall 2015 issue of Health Elevations.