

If there were an institution anywhere in the nation facing enormous challenges for which telehealth would seem to offer tantalizing solutions, it would be the Department of Veterans Affairs.
Tens of thousands of soldiers returning from physically and mentally crippling overseas deployments in need of ongoing health care. Rural and small-town heroes languishing hundreds of miles from care. A cashstrapped and oft-beleaguered federal administration always in search of more providers and more locations to serve a mushrooming clientele.
And so, indeed, the VA has for decades now tried to push the telehealth frontier in Colorado and across the rural and frontier West.
The early evidence is in black-and-white photos of 1950s-era VA psychologists in Nebraska trying a “two-way television link” for mental health counseling. Trace from there a direct line to the Eastern Colorado VA in 2016, more than 50 years later, placing new tablet computers directly in the homes of rural veterans so they can “see” their doctor by videophone from their living rooms.
In between, through that five decades of technology and health change, have been a relentless series of experiments and upgrades to the Eastern Colorado VA’s embrace of telehealth technology. One constant, said Marlys Withrow-Hill, the division’s home-based telehealth program manager, is empathy for what an ailing veteran goes through to get care.
“After a long drive, some veterans are so mad at their provider and the system that they won’t even fully reveal their conditions. They’re too angry to have a good visit,” Withrow-Hill said. “There are things people don’t bring up when they are distracted by anger, exhaustion and frustration. By the time they get in to see their provider in Denver, they are wiped. And then they still have to make it back home.”
Long veteran waiting times for appointments in Colorado and other states have prompted negative headlines and congressional queries. The Colorado Springs VA clinic, part of the Eastern Colorado unit and home to the state’s largest concentration of veterans, had wait times of at least 31 days for more than 10 percent of appointments in a six-month period in 2014-15, according to an Associated Press article. That made the clinic the 12th worst out of 940 VA clinics and hospitals nationwide, and far above the national average of 2.8 percent late appointments. Colorado, like other states, has a large inflow of veterans returning from overseas conflict, but also has a general population surge from a robust economy and attractive lifestyle, VA officials said at the time.

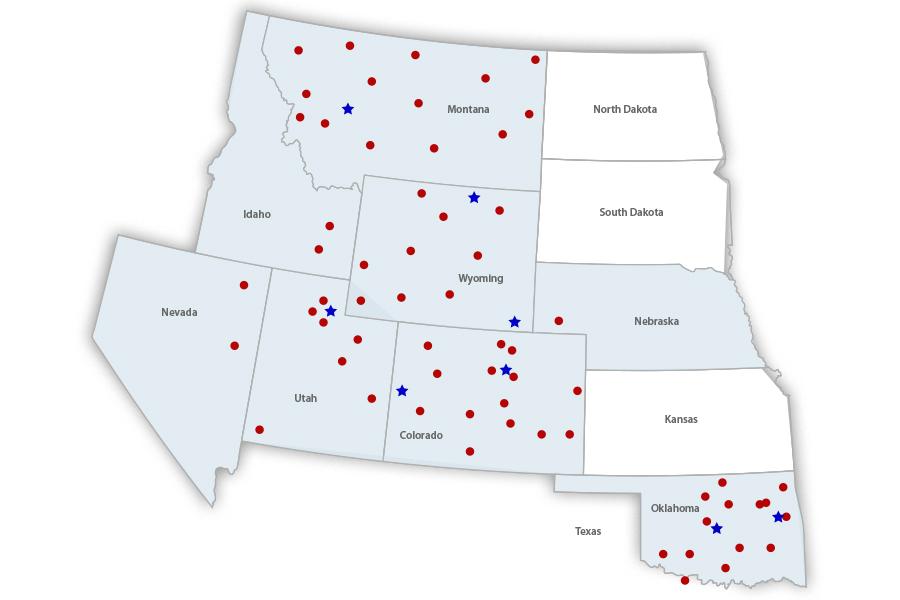
The VA’s Eastern Colorado unit alone takes care of 126,000 enrolled veterans. Glendale also houses the offices of the VA’s larger Region 19, encompassing hundreds of thousands more veterans in Montana, Oklahoma, Utah, Wyoming, Idaho, Nevada, Nebraska and the portions of Colorado not covered by the Eastern Colorado offices.
Just under 1,000 of those veterans are now using home telehealth in Eastern Colorado, and 33,000 use video telehealth at a local clinic to get specialty care from long distance, said Doug Van Essen, facility virtual health coordinator for the Denver VA Medical Center.
“We’ve seen it grow progressively throughout the years, and especially in the past three years it has blossomed,” Van Essen said.
Roy Hamilton is a Colorado Springs veteran who lost a leg in a motorcycle accident just before he left the U.S. Army. The upbeat Hamilton said it’s important to him to remain active, walking his dog, going on bike rides and water-skiing with an adaptive-abilities group. While he has seen the scheduling pressures on the VA at its local clinics, he said videoconferencing with VA doctors and consultants helped speed the fitting of a special waterproof prostheses.
Telehealth efforts in Colorado’s VA started in 2004, with high-risk veterans with chronic conditions and high volumes of care visits. Telemonitoring devices using their home phone lines could gather daily health readings and transmit them to a central office, which could then alter care accordingly.
Even that simple technology resulted in cuts in hospitalization of as much as 50 percent due to better care coordination.
Demand for video telehealth visits from satellite VA offices grew as “more and more soldiers returned from Iraq and Afghanistan, many with mental health factors,” Van Essen said. “One thing that made them uncomfortable was driving long distances and being at a large hospital with a large number of people.”
Improved and cheaper video technology made it possible for the VA to set aside remote clinic offices in Pueblo, La Junta or other locations, and set up live video visits with providers in Denver, Salt Lake City or other major medical centers.
The video visits can be a big boon for the providers, too. A specialist scheduled for a rotation in Pueblo could spend four hours or more of the day driving to and from the Denver home office. Technology in remote stethoscopes has improved, for example, to the point where a doctor listening remotely can hear more than an in-person visit in a noisy clinic.
“A primary care clinic in a tiny place like Salida can basically have all the access they would in Denver, given our specialist connections,” Withrow-Hill said.
Audiology is one of the booming specialties employing more telehealth. Hearing problems are rampant in veterans returning from loud training or combat zones. Few rural VA clinics can afford the specialty. But specially designed audiology “carts” in a small-town clinic can test a local veteran’s hearing and then offer critical adjustments to a hearing aid once it is delivered.
“The technology is now catching up with what we want to do,” Withrow-Hill said.
What she wants to do next is help the VA region dive even deeper into her favorite new technology: tablet computers allowing veterans to securely talk to their provider from the comfort of home. “For me, the greatest issue is still why are we dragging these patients into clinics when we could see them at home,” she said.
Veterans may qualify for the tablet computer connection by the severity of their condition, the remoteness of their home or various mental health needs. In addition to the live video link for appointments, the tablet can also be the portal for the veteran’s connection to medical records, test results and proactive health advice. Thirty thousand of the 90,000 actively seen veterans in Eastern Colorado’s division are using the personal health portal, Van Essen said.
The tablets can be loaded with various apps tailored to the veteran’s needs. Veterans with suicidal thoughts or expressions have started using “Hope Box,” an app that collects family photos, personal notes and other items that can remind the user of reasons to keep living.
More than 300 of the tablets have been set up in Colorado veterans’ homes, Withrow-Hill said, “and more are going out the door every day.”
One Vietnam-era veteran who was shown the new technology at a southeastern Colorado clinic called it “Buck Rogers-type stuff,” said VA Eastern Colorado spokesman Daniel Warvi.
The seemingly long wait for telehealth to move from science fiction to real life is ending now, Withrow-Hill said. “It’s here.”
VA Tries to Connect a Far-Flung Region to Embrace Telehealth
This article was originally published in the Fall 2016 issue of Health Elevations.